2430 SVD02 Claim or Line Level Prior Payment Information Required for this Patient
|
Rejection Message 2430 SVD02 Claim or Line Level Prior Payment Information Required for this Patient. 2320 AMT02 Claim or Line Level Prior Payment Information Required for this Patient. |
|
|
Rejection Details This rejection indicates that the patient has another payer listed as primary on file. |
|
|
Resolution Contact the patient for the missing insurance policy information. |
|
|
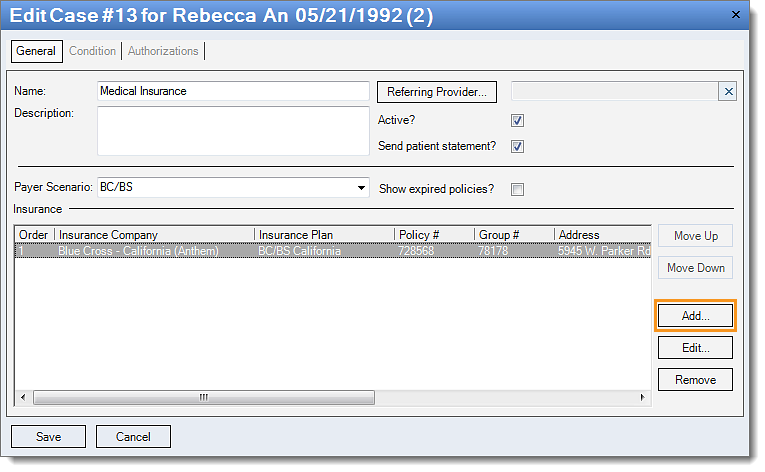
Follow these instructions below to add a new policy to the case:
Note: If there are multiple service lines, transfer the balance to the new policy for all affected claims. Then, rebill and resubmit all affected claims. |
 |